Dear readers, this piece about Sturgis and its aftermath has been weeks in preparation. We are sending it now because we believe that Sturgis was the largest of the super-spreader events that have occurred in the United States – half a million people without any restrictions. And we believe that learning can occur from examining what we now know about it and what we have learned about our government(s) from the outcomes. When I say governments, I mean states as well as the Trump administration, which is hosting the WH holiday reception in person on December 2.

Now let me add a few recent facts. The states around Sturgis have been on fire with COVID-19. The governors of those states are reacting differently: Readers can decide what constitutes a governor’s leadership success or failure. The hospitals are full in many places. Deaths and serious COVID illness numbers are setting daily records. The recent growth in the spread of the virus has been a multi-week event, with more to come.
We now know a lot about pre-symptomatic spread and asymptomatic spread. Here is a serious research effort on that subject: “The implications of silent transmission for the control of COVID-19 outbreaks,” https://www.pnas.org/content/117/30/17513.
Note that Donald Trump, Jr., admits testing positive, and his press release says that he’s asymptomatic. Note that he was at multiple events, and you know the Trump pattern of masking (not) and mitigation (not). Now look around at the Trump administration. Wikipedia has been tracking a Trump White House COVID casualty list, including a major events casualty list, though at the time of this writing the page does not yet include Don Jr. and Andrew Giuliani. See “White House COVID-19 outbreak,” https://en.wikipedia.org/wiki/White_House_COVID-19_outbreak. Looking back, though, the page is exhaustive and enlightening. The list of White House-related COVID infections starts with Donald Trump and Melania Trump and includes GOP Senators Thom Tillis, Mike Lee, and Ron Johnson; GOP Representative Matt Gaetz; Trump campaign manager Bill Stepien; RNC Chair Ronna McDaniel; former White House counselor Kellyanne Conway; former New Jersey Governor Chris Christie; Notre Dame president John I. Jenkins; Press Secretary Kayleigh McEnany; presidential advisor Stephen Miller; Chief of Staff Mark Meadows; and Housing and Urban Development Secretary Ben Carson. Altogether, at least 48 White House staff members or associates have tested positive for the coronavirus.
Dear readers, we have a few months to go before vaccines fully arrive. Letting your guard down now invites disease and risks death. Waiting a few months more for these marvelous vaccines to get into distribution is well worth the discipline and patience required. We’re getting close. Please don’t do a mini-Sturgis. BTW, in Florida, our governor, DeSantis, has the state wide open, and hospitalizations and cases are climbing daily. DeSantis is one of the governors who hasn’t learned. In my personal opinion he epitomizes leadership failure. He has presided over a million confirmed cases and more than 18,000 deaths of Florida residents. See the Florida Department of Health’s COVID Dashboard (https://experience.arcgis.com/experience/96dd742462124fa0b38ddedb9b25e429) and Rebekah Jones’s Florida COVID Action Dashboard (https://floridacovidaction.com).
Please be safe on Thanksgiving and throughout the holiday season. Now let’s get to Sturgis.
On August 6–15, nearly 500,000 motorcycle riders from every state in the nation converged on the little town of Sturgis, SD, for the town’s annual biker rally, an event that got its start in 1938 (https://www.sturgismotorcyclerally.com//timeline/). They were welcomed by South Dakota Gov. Kristi Noem, who told Fox News that the state was glad to host the rally. “We hope people come,” she said (“Gov. Noem on refusing to impose lockdown on South Dakota,” https://video.foxnews.com/v/6178249739001#sp=show-clips).
The public health outcome was readily predictable: COVID would spread among the participants and be carried home by them to spread farther. But in the rally’s wake we have seen a fierce debate over just how much additional sickness and death can be attributed to the rally. On one extreme we have the statement on the Sturgis Rally website that “fewer than 300 cases have been identified nationwide” as stemming from the rally (“2020 City of Sturgis Motorcycle Rally Update,” https://www.sturgismotorcyclerally.com/).
At the other extreme, a September report from the IZA Institute of Labor Economics, written by researchers from San Diego State University and IZA, estimated that 266,796 additional cases, or 19% of the 1.4 million new cases of COVID-19 in the United States between August 2 and September 2, 2020, were traceable to the rally, based on an analysis of anonymous cellphone data. The authors make the point that the huge disparity in numbers of reported infections “underscore[s] the extreme difficulty of using contact tracing alone to estimate the effect of massive, non-socially distanced gatherings on COVID-19 spread in the United States. The U.S. does not have universal contact tracing nor is universal testing required to identify asymptomatic cases.” (“The Contagion Externality of a Superspreading Event: The Sturgis Motorcycle Rally and COVID-19,” http://ftp.iza.org/dp13670.pdf)
The difficulty with Sturgis Rally contact tracing starts with the fact that many riders came from hundreds and even thousands of miles away, and they made many stops on their way to and from the rally. The difficulty of assigning COVID cases to the Sturgis event is further complicated when we note that South Dakota had also played host to President Trump’s Fourth of July rally, the state fair, and an early-September Mustang car rally in Sturgis. Bottom line: The state was averaging about 1,100 cases a day by early November, compared with fewer than 100 in much of August and September. (“A Motorcycle Rally in a Pandemic? ‘We Kind of Knew What Was Going to Happen’,” https://www.nytimes.com/2020/11/06/us/sturgis-coronavirus-cases.html). That figure is higher today.
The debate about studies and methodologies and contact tracing aside, the situation on the ground changed in South Dakota in the weeks that followed the rally:
[caption id="attachment_54301" align="aligncenter" width="750"]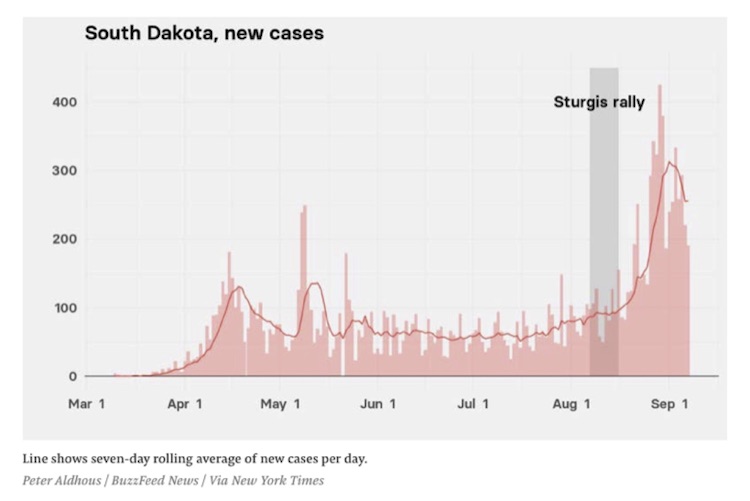 (Image Source: “The Sturgis Motorcycle Rally Was A Massive COVID-19 Superspreader Event, A New Study Claims,” https://www.buzzfeednews.com/article/peteraldhous/coronavirus-superspreader-sturgis-motorcycle-rally)[/caption]
(Image Source: “The Sturgis Motorcycle Rally Was A Massive COVID-19 Superspreader Event, A New Study Claims,” https://www.buzzfeednews.com/article/peteraldhous/coronavirus-superspreader-sturgis-motorcycle-rally)[/caption]
Another interesting way to look at the data is to spend a few seconds watching an animation that tracks the spread of COVID-19 in the US from March through early October. See https://www.savi.org/2020/10/09/animated-map-of-new-u-s-covid-19-cases-over-time/. Watch what happens in the weeks after the mid-August rally.
Here’s a snapshot from the animation for November 14:
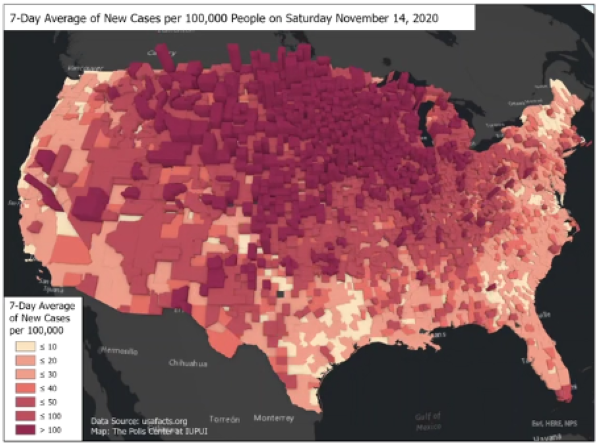
However it came to be, the resurgence of COVID-19 is severe in North Dakota, South Dakota, and Iowa, the states in closest proximity to Sturgis; and so it is tempting to posit a causal chain from the rally to the outbreaks. However, as epidemiologist and health economist Dr. Eric Feigl-Ding points out, a more significant factor in the severity of the resurgence may be failure by the governments of these states to maintain forceful virus containment efforts or to implement basic measures like mask mandates. (https://twitter.com/DrEricDing/status/1329439169031057408)
So, how much can be expected of state governments, particularly in states where the populace is strongly averse to pandemic-control measures AND when COVID-19 policy is scattershot or missing altogether at the federal level? For instance, in North Dakota, Gov. Doug Burgum announced on Nov. 9 that the state would allow healthcare workers who have tested positive for COVID-19 to continue working if they don’t show symptoms. That decision was strongly criticized by the American Nurses Association, the North Dakota Nurses Association, and the state’s Emergency Nurses’ Association; but the state hastened to point out the that the policy was recommended to them by the U.S. Centers for Disease Control and Prevention (CDC), for use in crisis situations as a way to deal with staffing shortages. (“North Dakota says health workers with COVID-19 who don’t show symptoms can keep working,” https://www.cbsnews.com/news/north-dakota-covid-19-nurses-healthcare-workers/)
Events caused Governor Burgum to reverse himself. After months of resisting a statewide mask mandate, on Nov. 13 Gov. Burgum ordered that masks be worn statewide: “The Dakotas are ‘as bad as it gets anywhere in the world’ for COVID-19,” https://www.usatoday.com/story/news/health/2020/11/14/covid-19-north-south-dakota-masks-kristi-noem/6237635002/.
The lack of coherent federal policy leaves even states with strong COVID-control programs vulnerable to the actions of states that are lax or resistant:
In many ways, Sturgis is an object lesson in the patchwork U.S. response to a virus that has proved remarkably adept at exploiting such gaps to become resurgent. While some states and localities banned even relatively small groups of people, others, like South Dakota, imposed no restrictions – in this case allowing the largest gathering of people in the United States and perhaps anywhere in the world amid the pandemic and creating huge vulnerabilities as thousands of attendees traveled back home to every state in the nation. (“How the Sturgis Motorcycle Rally may have spread coronavirus across the Upper Midwest,” https://www.washingtonpost.com/health/2020/10/17/sturgis-rally-spread/)
A study on the effects of the Sturgis Rally on the incidence of COVID cases in Minnesota was published by the CDC itself, on November 20. While the study results are not eye-opening – 51 confirmed Sturgis-associated cases, 21 secondary cases, and five tertiary cases were identified in Minnesota residents; four patients were hospitalized, and one died – and while the study’s central conclusion is a bit of a yawner (“These findings support current recommendations for mask use, physical distancing, reducing the number of attendees at gatherings, isolation for patients with COVID-19, and quarantine for close contacts to slow the spread of SARS-CoV-2”) – the study’s authors do concur that their research “demonstrate[s] the rationale for consistent mitigation measures across states.”
In the final analysis, the United States is just a collection of some 330 million people. Some are doing their best to self-govern. Others don’t care or behave as if there is no threat. The fracture we are enduring in our body politic has left us in the midst of a worsening pandemic where many citizens and even some of their elected leaders feel they are better off ignoring or repudiating the advice of medical experts. If such people want to congregate mask-free in large numbers and then refuse to self-quarantine or to be tested for COVID-19, then they are going to do so. “Don’t tread on me” – even if it means my vaunted freedom carries with it the cost of millions sickened and thousands killed.
We’ll give Josh Michaud, an epidemiologist with the Kaiser Family Foundation, the final word: “Holding a half-million-person rally in the midst of a pandemic is emblematic of a nation as a whole that maybe isn’t taking [COVID-19] as seriously as we should” (“How the Sturgis Motorcycle Rally may have spread coronavirus across the Upper Midwest,” https://www.washingtonpost.com/health/2020/10/17/sturgis-rally-spread/).
We have yet to do what it will take to stem the tide of infections. Almost 20% of the nation’s hospitals are overwhelmed and understaffed as cases, hospitalizations, and deaths trend higher at alarming rates all across the US (“1,000 U.S. Hospitals Are ‘Critically’ Short On Staff — And More Expect To Be Soon,” https://www.npr.org/sections/health-shots/2020/11/20/937152062/1-000-u-s-hospitals-are-short-on-staff-and-more-expect-to-be-soon). As of yesterday, “27% of all inpatients beds in the U.S. are occupied by Covid-19 patients. Nevada 57% of beds. Connecticut and New Mexico just under 50%. Colorado, Illinois, Indiana, Michigan, Minnesota, Missouri, Rhode Island and Wisconsin above 33%.” Source: Mark Van Sumeren, COVID-19 Report, 11-23, Issue #219.
As of today, MEDPAGE reports ICU beds available “in Minnesota are down to single digits”; “Michigan Hospitals asked exposed but asymptomatic employees to still come to work”; “Wisconsin extends its mask mandate for 60 days”. An Arizona Emergency Room Doctor Cleavon (@Cleavon_MD) tweeted “No ICU BEDS! When our rural hospital ICU is full, we medevac patients to different hospitals across the state, BUT NOT TONIGHT, because there were NO ACCEPTING HOSPITALS, so for an entire 12 hour shift we managed ICU patients, while treating other emergencies. As an ER doc, I’m worried because aside from hypoxic patients we are still seeing a lot of aforementioned HIGH ACUITY emergencies and staff getting sick. There are only so many available ICU doctors and nurses to take care of ICU patients. These are very skilled professionals with knowledge in critical care.” Dr. Cleavon ended his thread with this: “ WTF is going on in this country? Is anyone going to do anything to stop the 2000 people dying a day? All this talk about the election… but REAL people are dying and our hospitals are overwhelmed. ZERO help! Endless patients! I’ve never seen such cowardice in my life.”
We have a lot to contemplate on Thanksgiving. Please be safe.
David R. Kotok
Chairman of the Board & Chief Investment Officer
Email | Bio
This commentary was originally published via MailChimp. To see it or subscribe, follow this link: Check it out.
Links to other websites or electronic media controlled or offered by Third-Parties (non-affiliates of Cumberland Advisors) are provided only as a reference and courtesy to our users. Cumberland Advisors has no control over such websites, does not recommend or endorse any opinions, ideas, products, information, or content of such sites, and makes no warranties as to the accuracy, completeness, reliability or suitability of their content. Cumberland Advisors hereby disclaims liability for any information, materials, products or services posted or offered at any of the Third-Party websites. The Third-Party may have a privacy and/or security policy different from that of Cumberland Advisors. Therefore, please refer to the specific privacy and security policies of the Third-Party when accessing their websites.
Sign up for our FREE Cumberland Market Commentaries
Cumberland Advisors Market Commentaries offer insights and analysis on upcoming, important economic issues that potentially impact global financial markets. Our team shares their thinking on global economic developments, market news and other factors that often influence investment opportunities and strategies.
